Brief recap of what I did this summer.
16 June: MS1 ended (whoo)
17 June – 21 June: kicked it in Santa Barbara, LA, and Big Bear, where I climbed Sugarloaf Mountain to train for Mt. Kilimanjaro
22 June: flew from LAX à Amsterdam à Kilimanjaro
23 June – July 3: climbed Mt. Kilimanjaro with Peak Planet
July 3 – July 10: flew to Addis Ababa and toured Ethiopia’s northern route of historical sites
I boarded an Ethiopian Airlines flight at Bole International Airport in Addis Ababa bound for Entebbe International Airport, the major air traffic hub of Uganda located near its capital city, Kampala. I spent the flight savoring reminisces from my holiday hiking Mt. Kilimanjaro and immersing myself in Ethiopia’s history and culture. Though I had enjoyed my time off, it had been over three weeks since my brain had been engaged in work mode and I was excited to finally bring my (admittedly meager) faculties to bear on an academic project.
I would spend seven weeks (10 July – 26 August, 2017) in rural Uganda conducting global health research on two mosquito-borne illnesses: malaria and dengue. As I mentioned in a previous post, I was thrilled by this chance to investigate infectious diseases in the field. This opportunity was bestowed upon me through the Global Health Academic Concentration (GHAC) at UC San Diego School of Medicine. This program selects a few medical students per class and provides them with funding to complete a global health research project in the summer between MS1/MS2 and an international clinical rotation during MS4. GHAC provides medical students with exposure to the rewards and challenges of working in low-resource settings with the hope that they will pursue careers in global health.
I selected this project for two reasons: my vested interest in infectious diseases and a specific desire to experience first-hand the negative impacts of malaria. My high school years at Bellarmine College Prep seeded a personal drive to pursue a career serving the needy (our motto was Men for Others, and associated feel-good twaddle). This seed began to germinate in my freshman year at Haverford College when I learned about the disproportionate suffering that infectious diseases inflict upon impoverished populations, the potential for disaster posed by superbugs, and the field’s explainable-yet-inexplicable relegation to the backburner of Western medicine. I recognized infectious diseases as a beleaguered and understaffed field in which I could certainly help the poor and possibly help mankind. My desire to join the fight against infectious diseases has carried me through several research labs around the world and continues to influence my professional direction in medical school.
I was specifically interested in malaria because of my background studying the disease. Malaria is an ancient disease that has plagued mankind since time immemorial and continues to inflict considerable morbidity and mortality worldwide. It is considered one of the Big 3 infectious diseases alongside HIV/AIDS and tuberculosis. Last summer, I did a rotation in a basic research lab at UCSD where I investigated the genetics of the Plasmodium parasites that causes malaria. I enjoyed the rotation and continued to work in the lab during my first year in medical school. While the scientist within me was content, the physician within me yearned to study the bio-social aspects of malaria. This is difficult to do in the USA because there are nearly no people with malaria in the USA. The handful that do usually have a recent travel history to a malaria-endemic country…like Uganda. Thus, I jumped at this opportunity to interrogate malaria in the field because it would enable me to complement my molecular knowledge of the Plasmodium parasites with personal observations of how the disease impacts the lives of Uganda’s indigent rural population.
I would be involved in two separate projects. I would take the lead on a small study focused on tracking pharmacy sales of anti-malaria drugs in rural villages in western Uganda. I would also function as a consultant and itinerant supervisor of a much larger study investigating dengue, another mosquito-borne infectious disease. My time would be separated into two phases: I would spend the first two weeks shadowing my principal investigator (PI) and the latter five weeks flying solo.
My PI and mentor for the summer was Dr. Ross Boyce MD, MSc. I Googled him and was struck by his career path. He had attended Davidson College (a small liberal arts college like Haverford), joined the army after college and served in Iraq (I learned after the fact that he was a Special Forces sniper, holy s**t), taken a year off in medical school to complete a MSc at the London School of Tropical Medicine and Hygiene, completed his residency in internal medicine at Massachusetts General Hospital, and was currently finishing his fellowship in infectious diseases at UNC Chapel Hill. In short, I knew I would learn a lot by interacting with him.
Week 1 (July 10-16) – Mbarara
Dr. Boyce and I both flew into Entebbe and spent the night at the Airport Guest Lodge. In the morning, we drove west to Mbarara, the major city of Uganda’s western region, where we would spend our first week. The trip was 5.5 hours and took us through the equator, where we stopped at a shop that sells artwork and donates its proceeds to a home for HIV+ orphans.


 There are two main ethnic groups in the western region of Uganda, of which Mbarara was once the de-facto capital. The first (and numerically greater) group are the Bairu, who were traditionally agriculturalists. The second group are the Bahima, who were traditionally cattle herders. Despite being numerically smaller in number, the Bahima were historically wealthier, better educated, and more influential than the Bairu. This division is largely rooted in Uganda’s previous status as a colony/protectorate of the British empire. Selecting a pet/puppet minority and bestowing them with wealth and power was a common strategy employed by colonialists. It enabled the tiny numbers of white overlords to exercise control over their multitudes of black subjects and keep them divided along man-made gaps of resentment and sectarianism. Anyway, this statue shows a woman and child of the Bahima, denoted by their standing on a foundation made of a longhorn cattle. The current president of Uganda, Yoweri Museveni, is Bahima.
There are two main ethnic groups in the western region of Uganda, of which Mbarara was once the de-facto capital. The first (and numerically greater) group are the Bairu, who were traditionally agriculturalists. The second group are the Bahima, who were traditionally cattle herders. Despite being numerically smaller in number, the Bahima were historically wealthier, better educated, and more influential than the Bairu. This division is largely rooted in Uganda’s previous status as a colony/protectorate of the British empire. Selecting a pet/puppet minority and bestowing them with wealth and power was a common strategy employed by colonialists. It enabled the tiny numbers of white overlords to exercise control over their multitudes of black subjects and keep them divided along man-made gaps of resentment and sectarianism. Anyway, this statue shows a woman and child of the Bahima, denoted by their standing on a foundation made of a longhorn cattle. The current president of Uganda, Yoweri Museveni, is Bahima.
 One of the main roads in Mbarara early in the morning. The city was crowded and polluted, with cars and boda boda’s (motorcycles) whizzing by. This was one of the few streets with sidewalks. One had to be situationally aware on most of the other side streets because cars and bodas would whiz by at high speeds right next to you.
One of the main roads in Mbarara early in the morning. The city was crowded and polluted, with cars and boda boda’s (motorcycles) whizzing by. This was one of the few streets with sidewalks. One had to be situationally aware on most of the other side streets because cars and bodas would whiz by at high speeds right next to you.

Dr. Boyce was working with members of the MUST faculty to begin a study that aimed to determine whether dengue is present in Uganda. Dengue is a virus that, like malaria, is carried by mosquitos. It also causes symptoms (e.g., high fever, body aches, weakness, etc.) that are difficult to distinguish from malaria. Thus, dengue is often misdiagnosed as malaria, especially in poor malaria-endemic countries like Uganda. Dengue infections are usually asymptomatic; however, when symptoms do appear they can be terrible (dengue is also known as “break bone fever” because the body aches and fever are just that bad). In some rare cases, dengue can cause a fatal hemorrhagic fever which causes massive internal bleeding and can send one into shock. There are no specific treatments for dengue, so patients are usually given supportive care like fluids and painkillers.
There is a body of circumstantial evidence suggesting that dengue is present in Uganda. First, every single country that shares a border with Uganda has dengue. Second, Western travelers to Uganda have come down with dengue when they return to their respective countries (hopefully I won’t be one of them). Third, the mosquito that carries dengue, Aedes aegypti, is present in Uganda. Fun fact: this mosquito also carries the infamous Zika virus, which was first isolated and described in Uganda in the 1950’s. It’s a pretty sure bet that dengue is here, someone just has to prove it. And that someone is hopefully Dr. Boyce and the MUST team.
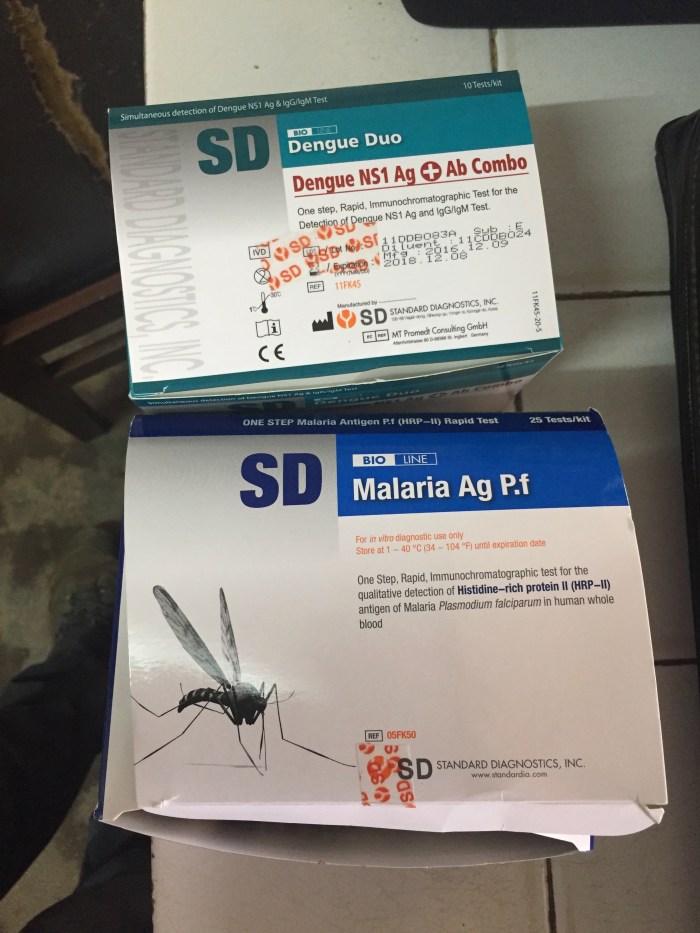
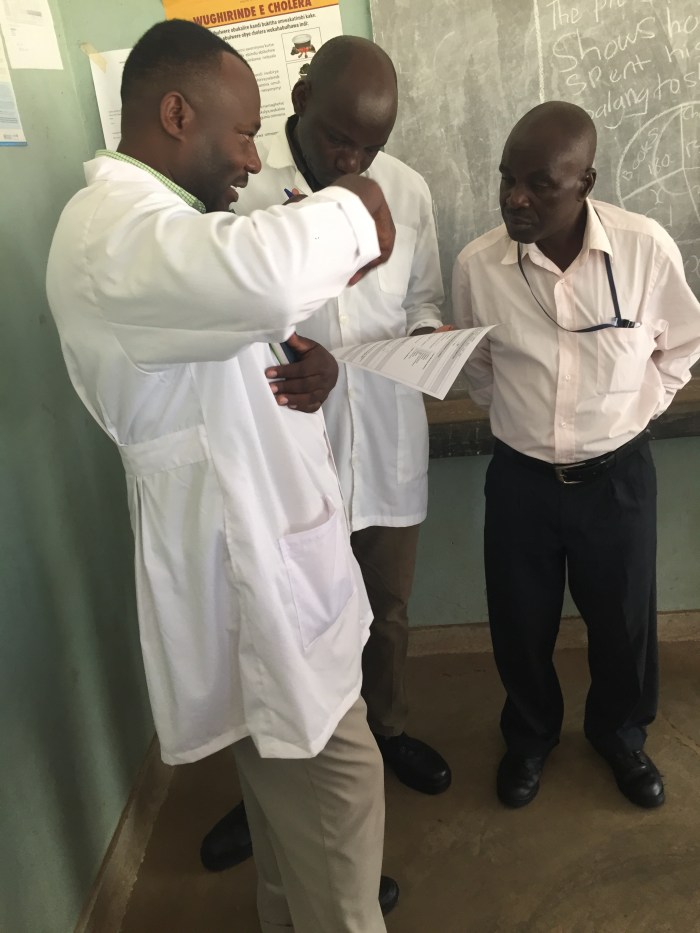
During that first week in Mbarara, I spent most of my time sitting through meetings where we talked about what needed to be done to start and finish the dengue study. I mostly observed and didn’t say much. We met and had meals with Dr. Edgar Mulogo and Dr. Moses Ntaro, who were professors at MUST and had been collaborating with Dr. Boyce since he first started working in Uganda four years ago as a MGH resident. We also met with Dr. Mugabe, who was the director of the outpatient department at Mbarara Regional Referral Hospital, the large (by Ugandan standards) teaching hospital attached to MUST where the study would take place. We also had dinner with a representative from a biotechnology company that had donated malaria and dengue field diagnostic kits called RDTs (rapid diagnostic tests) that are cheap and have a quick turnaround time. These RDTs are thus ideal for diagnosing diseases in low-resource settings in the field.
The dengue study would take place at three sites: Mbarara, Kasese, and Bugoye. Mbarara is a large urban city, Kasese is a semi-urban town, and Bugoye is a rural village. The Aedes aegypti mosquito likes to breed in tiny pools of water that accumulate in trash (e.g., like a puddle inside of a tire) and is typically found in urban environments. Dr. Boyce predicted that Mbarara and Kasese would have the highest rates of dengue since they are respectively urban and semi-urban.
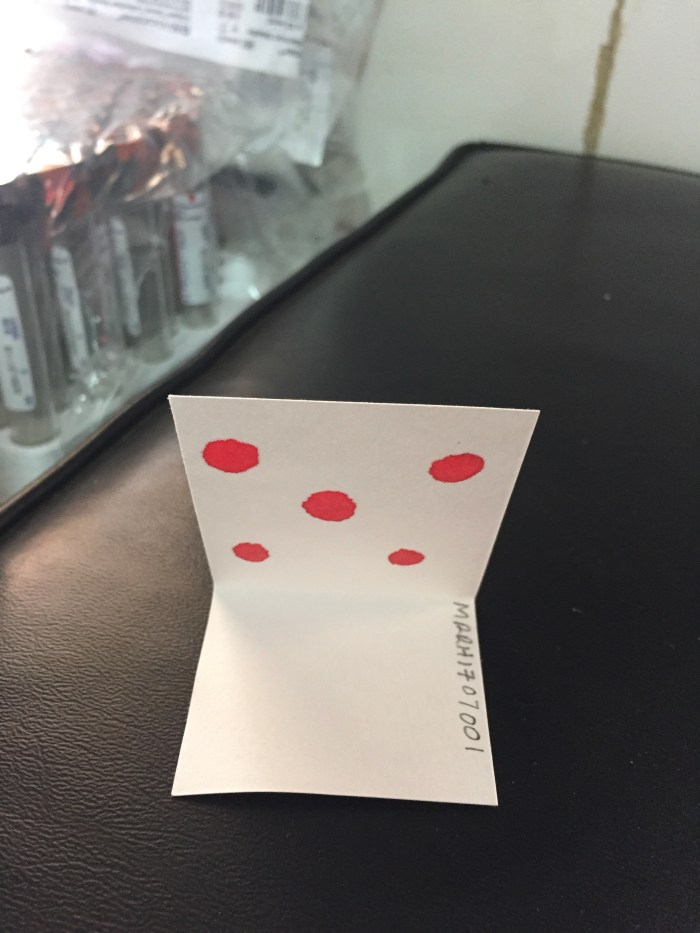
The goal of the study was to identify dengue as a culprit behind non-malarial fevers in children. To do this, patients between the ages of 1-18 years presenting with fevers at each of the sites would be consented into the study. They would have a small sample of blood drawn by finger-stick. The blood would be placed on filter paper to create blood smears for later testing and also be tested using a malaria RDT. If their blood was positive for malaria, they would be given anti-malaria drugs and exit the study because their fever was caused by malaria, not dengue. If their blood was negative for malaria, they would have another finger-stick blood draw and their blood would be tested using a dengue RDT. This way, we would be able to define what proportion of fevers NOT caused by malaria are caused by dengue and thus be able to calculate the burden of dengue in Uganda.
I helped the MUST team set up the laboratory for the study and was able to observe them do a dry run using a few sample RDT kits provided by the biotech companies. Dr. Ross had brought these RDT kits (as well as gloves, blood vials, filter paper etc.) from the USA to help facilitate these practice dry runs.




Dr. Boyce also arranged for me to spend a morning on rounds with an Ugandan attending physician at Mbarara Hospital named Dr. Okello. Dr. Okello gave me a brief tour of their facilities and explained the day-to-day of the hospital. Mbarara Hospital’s full title is Mbarara Regional Referral Hospital (MRRH). It is the largest hospital in Uganda’s western region and has a wide catchment area. All the hospitals/health centers in the area send their most challenging cases to MRRH. I noted that the hospital has the following: emergency department, ICU, STI clinic, oncology clinic, pharmacy, inpatient/outpatient wards. There are probably a few more parts that I missed. As you can see from the picture, the hospital is open complex composed of 1-3 story buildings that are spread apart from each other. It was very crowded, with many patients and their families jostling in packed waiting areas or sitting outside on the ground, under trees, on curbs, on the grass, anywhere there was an open space.



MRRH, like many hospitals in poor countries, is severely understaffed. There are usually only 2 nurses and one resident per ward, and each ward has 40 beds. However, sometimes patients lay two to a bed, and some patients even lay on the ground underneath beds and between beds. Routine care of patients is severely lacking. Many patients are cared for by their relatives, who feed and wash them and try to get the nurses and doctors to give them their medications. Sometimes, the relatives are even charged with administering medications to their loved ones. This is simply because the hospital is so understaffed. The nurses can’t possibly take care of the basic needs of their multitude of patients. The signage (where it exists) is poor, and many patients get lost.
The hospital was dirty, stuffy, malodorous, crowded, and dim. I remember walking through one of the hallways and catching a glimpse of a patient with a gaping wound in his forearm laying on the ground. I could see clearly his glistening bone underneath and the blood that was oozing out of the wound. I saw many patients lying listlessly on the ground, with their worried relatives standing over them as they waited to be seen. Flies and other flying insects buzzed freely into the wards through open windows. I had to remind myself that this was one of the biggest hospitals in Mbarara and presumably the conditions here were better than some of the smaller hospitals in the western region.
Dr. Okello left me with a resident who took me on rounds of the male inpatient ward. The only people rounding were the resident and two nurses. Since they were so understaffed and underequipped, I lent one of the nurses my stethoscope and helped record vital signs and other notes in the patient’s charts. The charts consisted of dilapidated notebooks made of a few ratty sheets of binder paper stapled together. I noticed that the various caretakers who had made notes in the chart all had differing handwriting (most of it illegible), which was further exacerbated by the lack of hard surfaces for them to write on. The resident balanced the notebook chart on his thigh and scrawled his assessment and plan.
These were some of my observations about the conditions of the patients and the diagnoses/diseases they had, based on what I gleaned from reading the chart and interacting with the resident:
- Seizure secondary to a motorcycle accident and associated head trauma
- Pneumonia secondary to a bacterial infection (the patient had a tube inserted into his left lung, which was leaking milky pus into a container)
- Cerebral malaria (the patient was glassy eyed and unresponsive)
- Chronic kidney disease (the patient had a swollen peritoneum which was painful to light palpation. Apparently there is one dialysis machine in the entire western region)
- Lymphoma (patient was septic and leukopenic, had hypersplenomegaly. He needed antibiotics urgently but was not able to afford it)
- Crytococcal meningitis (opportunistic infection of a person with advanced HIV/AIDS)
- HIV + tuberculosis (patient was on RIPE therapy for TB)
- Prostatic adenocarcinoma and urosepsis (sepsis was due to an infected catheter)
- HIV + severe malaria (coartem had mostly cured the malaria infection but the patient was still severely immunocompromised. I noticed that they had not done CD4 counts/viral loads for any of the HIV patients and were treating on clinical principles).
When I asked the resident what his plan for the patients were, he told me that he would prescribe them with appropriate medications but that the pharmacy was currently out of most medications. Thus, the patients (or really their families) would have to go other pharmacies to get the treatments they needed. However, many of the patients could not afford some of the treatments and had poor prognoses.
While I expected such poor conditions and severely ill patients, it was still sobering and shocking to experience the abysmal conditions in Mbarara Hospital. I also thought back to how empty the hospital pharmacy had been when Dr. Okello showed me it. The pharmacy for the entire hospital had only a handful of containers on the shelves (no more than 10-15) and had only one person working in it at the time I saw it. Dr. Okello confirmed that there were constant pharmacy drug shortages and that the hospital would often run out of such basic materials as gloves.
I was also told a story that exemplified the realities of medicine in low-resource settings. There was supposed to be a scheduled power outage in Mbarara, which would also affect the hospital. The hospital administrators tried to ensure that the outage would not affect the ICU patients, who needed ventilators to stay alive. They had arranged for the power outage to only affect one wall of the ICU room at a time. Thus, all they had to do was move the patients from the side of the ICU that was out of power to the side with power, and then switch them back when the power outage switched sides. However, their orders were lost in translation and the patients were left where they were. All the ICU patients on ventilators ended up dying, and the hospital staff just shrugged it off. So it goes.
Perhaps the only good news I heard was that the hospital had plentiful stocks of HIV drugs. This is because PEPFAR (President’s Emergency Plan For AIDS Relief) has provided ample funding for HIV global health interventions. PEPFAR was started by President George W. Bush and is regarded as one of his most successful legacies. HIV is alternatively referred to as ISS (Immune Suppressive Syndrome) in Uganda. This is because the word HIV had (and still has) enormous stigma attached to it in the country. People would refuse to interact or touch patients infected with HIV, so the healthcare community took to calling it ISS to protect those infected with HIV from being shunned by society.
I concluded my week in Mbarara with a bout of food poisoning. Luckily, I succumbed to the friendly neighborhood bacterial (or viral) fauna on a Friday, so I could spend the weekend in bed recovering without missing anything work-related. People close to me have noted the irony inherent in the image of a sissy like me, with a lackluster immune system who gets sick several times a year, working in a place infested with the world’s most dangerous pathogens. Anyway, I just took some Pepto Bismol and toughed it out.
Week 2 (July 17-23) – Bugoye
After my weekend spent recovering from my unfortunate encounter with the native Ugandan bacteria/viral flora, Dr. Boyce and I got on a car and drove for 3.5 hours to Bugoye, the village where I would be living for the rest of the summer and where my main project, the one focusing on malaria, would take place. We passed through Queen Elizabeth Park on the way to Bugoye, which is famed as a safari destination. We saw a few animals along the way:







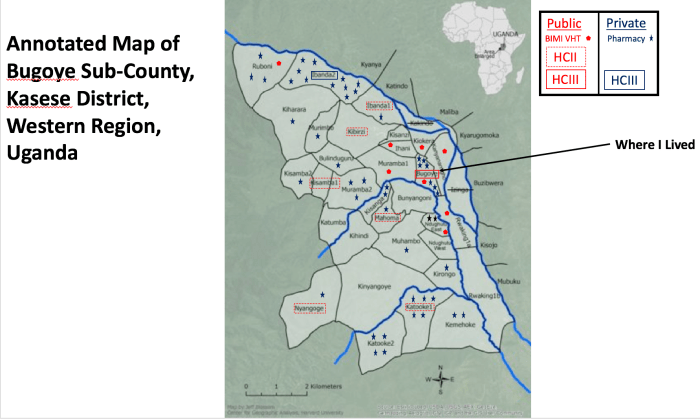
We finally arrived at our destination, Bugoye Health Centre III (HC III), a public health facility funded by the Ugandan Ministry of Health. It is located in the rural village of Bugoye and serves the larger Bugoye sub-county, which is in the Kasese District of western Uganda. Bugoye is at an elevation of roughly 4,000 feet, and the entire sub-county is located in the foothills of the Rwenzori Mountains (more to follow), about 10 kilometers east of the border with the Democratic Republic of the Congo (DRC). The enormous Rwenzori Mountain range acts as a natural border between Uganda and the DRC. The population of Bugoye sub-county, and thus the referral base of the HC III, is 50,000 people. The population is stable and there is very little migration. The health center has a monthly influx of 800-1,200 patients. The regional malaria prevalence among children <5 years old in 2009 was 42.7%. I was told upon arrival that they had observed a whopping 60% malaria prevalence in under 5s in May 2017.

Before I explain the number rating of health centers and the overall healthcare infrastructure in Uganda, I have to first describe the way Uganda’s population is organized. The healthcare infrastructure is designed to provide services to these population quanta.
Classification of Population Quanta:
Village (2×2 kilometers) –> 1,500-2,000 people (e.g., Ruboni village is in Bugoye sub-county)
Parish –> 5-6 villages (~10,000 people)
Sub-county –> 5-6 parishes (~50,000 people)
County –> uncommon classification, most sub-counties are lumped into districts.
District –> collection of several sub-counties (e.g., Bugoye sub-county is in the Kasese district)
Region –> swathe of land in Uganda (e.g., the Kasese district is in Western Uganda)
Classifications of Uganda’s Community Health Infrastructure:
Uganda’s community health infrastructure is composed of health centers ranked from I-IV.
HC I –> at the village level. A HCI isn’t actually a building, it is a VHT (village health team) that is composed of two volunteer community health workers per village. They are responsible for basic health interventions like handwashing campaigns, diagnosing high-impact diseases (i.e., pneumonia, diarrhea malaria) using rapid diagnostic tests (RDTs), and dispensing basic medications (i.e., antibiotics and Coartem, an anti-malaria drug)
HC II –> at the parish level. One building staffed by a small team of nurses and nursing assistants who are responsible for diagnosing diseases using RDTs and dispensing appropriate medications. They have a wider range of diagnostic tests and medications available than HC I’s.
HC III –> at the sub-county level. Usually a collection of buildings staffed by a team of nursing assistants, nurses, physician assistants who operate an in-patient ward, maternity ward, outpatient clinic, and diagnostic lab. The labs are staffed by lab technicians and lab assistants and offer an even wider array of diagnostic services (e.g., TB sputum tests, blood smears for malaria)
HC IV –> county/district-level health center that is essentially a larger and better-equipped HC III.
Regional referral hospital –> Large hospitals that receives referrals from HC I-IVs. For instance, Mbarara Regional Referral Hospital (MRRH) is the largest hospital in the western region of Uganda and has a wide catchment area.


The health center is a tidy compound of one-story buildings located next to the main dirt road cutting through Bugoye village. The health center has an in-patient department (pediatric, men, women wards), a maternity ward, an outpatient department, a laboratory, pharmacy/dispensary, and immunization clinic. Most of the above facilities are open M-F, with business hours from 8:30am-5pm. All medications and labs at the health center are free, though patients must make a small co-pay to be seen by the hospital staff. On peak days, patients are still waiting to be seen at closing time, whereas on light days the clinic gets quiet around 2-3pm but remains open till 5pm. Most visitors to the health center are women and children; men do not generally go to the clinic unless they are extremely ill. Below is the clinic’s general weekly schedule:
Monday –> general clinic, very crowded, peak day
Tuesday –> HIV ART (antiretroviral therapy) clinic, not as crowded because non-HIV infected know its ART clinic and come in on other days. The prevalence of HIV in Bugoye is 8%, which is lower than the national average.
Wednesday –> general clinic, very crowded, peak day
Thursday –> Hypertension clinic, not as crowded because non-HTN clinic patients come on other days
Friday –> few people because it’s close to the weekend
There are specialty clinics for tuberculosis diagnosis/drug dispensation (run for an entire week sporadically if a TB outbreak has been detected, though TB is generally not a problem in Bugoye), a circumcision clinic (once a week sporadically), and an ophthalmology clinic (once a week sporadically).











 This is on a light day
This is on a light day



- Beds in the in-patient ward, I tried to take a picture of one that was empty. This was much nicer than Mbarara, where I didn’t take pictures to respect the patients. The inpatient ward has 10 women beds and 4 men beds. It usually overflows with malaria patients.






I spent most of the week sitting through even more meetings and getting acquainted with the staff of Bugoye HC III. They were all very nice and I knew I would be welcomed for the rest of the summer once Dr. Boyce left. They all also spoke highly of Dr. Boyce and some of them were obviously very close to him.
We also spent a significant portion of the week in the nearby city of Kasese, the major city in the Kasese district, of which Bugoye is a part. We were there to help set up the third arm of the dengue study at Kasese’s Health Centre III. Besides meeting with the staff at the health center, we made a trip to see the Kasese district chairman and, as Dr. Boyce put it, “kiss the ring.” Essentially, we were making a courtesy call to the chairman of the Kasese district to tell him what we were trying to accomplish in our study at the health center. As usual, he was on African time (it’s a thing) and arrived late to the meeting. This happened at a lot of the meetings I sat through, the Africans would arrive egregiously late and apologize and things would begin as usual. This was certainly an interesting cultural phenomenon that was wildly divergent from customs in America, where arriving on time for an official meeting is expected.






Finally, near the end of the week I was able to head into the field around Bugoye and begin my main project. Dr. Boyce had asked me to take the lead on a study that sought to determine how many anti-malarial drugs are dispensed through private-sector drug shops in Bugoye sub-county. We wanted to compare the numbers and types of anti-malarial drugs that patients obtain through the private-sector (i.e., drugs sold by private individuals who run drug shops in the villages) to the numbers and types they obtain through the public-sector (i.e., drugs dispensed free of charge through Bugoye sub-county’s HC I, II, and III’s). The goal of the study was to determine how many anti-malaria drugs are being obtained outside of public-sector health centers in Bugoye sub-county.
One would presume that most people infected with malaria would seek treatment at public-sector health centers because they are free and are run by certified medical professionals. However, there are only a small number of health centers in the entire sub-county, and it is sometimes difficult or expensive for patients to get to them. It is much more convenient for people who live far away from a health center to visit drug shops in their local villages, even if they have to pay for the drugs. So, the pro for public-sector health centers is that they are free or very cheap. The con is that they are not accessible for some people. The pro for private-sector drug shops is that they are close and convenient to get to. The con is that one must pay for one’s medications. Dr. Boyce has long assumed that most patients get their anti-malarial drugs through the public-sector because they are free. However, he doesn’t know for sure, and if that isn’t the case, then it will be important to include private-sector drug shops in any future public health interventions that target malaria and other diseases in the sub-county.
Before I dive into the details of my adventures in the field, I want to provide my readers with a brief introduction to malaria. Malaria is an ancient mosquito-borne infectious disease that is caused by parasitic worm-like protozoa that belong to the Plasmodium family. There are five species of Plasmodium that cause malaria: P. falciparum, P. vivax, P. ovale, P. malariae, and P. knowlesi. The deadliest of the five species is P. falciparum. The mosquito vector that transmits malaria is the Anopheles mosquito. Symptoms of malaria include fever, malaise, headaches, shivering, myalgia/arthralgia, and vomiting. Patients with severe malaria can develop yellowing of the skin, seizures, and coma. These symptoms manifest after 10-15 days because of the long incubation period of the parasites in the human host’s body
Plasmodium parasites have a complex life cycle. When the Anopheles mosquito bites a human and sucks up a blood meal, it also transmits sporozoites (a developmental stage of the Plasmodium parasites) living in its saliva into the human host’s body. Most of the sporozoites are trapped in the skin and eventually destroyed by white-blood cells called macrophages. However, a few of them (as few as 10-12 parasites) are able to travel through the blood and make it to the liver, where they then infect and set up shop in liver cells. Each sporozoite transforms its infected liver cell into a factory that produces thousands of a different stage in the life cycle called merozoites. While living in the liver cell, the merozoites are safely hidden from the body’s immune system. Once the parasites have produced sufficient numbers of themselves and exhausted the resources of its host cell, they cause their host cell to pop free of its cellular anchors and float into the blood supply of the liver. The engorged liver cell travels into the bloodstream where it bursts, releasing thousands of merozoites that then go on to infect red blood cells. This is called the blood stage of malaria infection and is when all the nasty symptoms start to manifest, usually 10-15 days after the fateful mosquito bite. The merozoites infect the red blood cells and turn them into factories wherein they undergo rapid asexual division and produce even more merozoites. The red blood cells violently explode and release a flood of merozoites that then go on to infect even more red blood cells in an ever-increasing cascade of cellular carnage that leads to the nasty symptoms of malaria. The blood stage is cyclical because it follows the parasite’s life cycle, which is the reason why patients vacillate between feeling feverish (when their red blood cells are exploding and releasing parasites) and feeling relatively better (when the parasites have found new host cells and are replicating quietly inside them. The calm before the storm, if you will).
People afflicted with malaria are not contagious to other humans (unless you give yourself an IV infusion of their blood, in which case someone should nominate you for the Darwin Awards). However, they can transmit the parasites to hungry mosquitos that bite them, which can then go on to infect even more human hosts. The transmissible forms of the Plasmodium parasites are called gametocytes, they are formed by a small number of merozoites during the blood stage that undergo sexual (rather than asexual) division.
There are a number of effective drugs available to treat malaria. The gold-standard are the ACTs, artemisinin combination therapies. The artemisinins were originally isolated and described by Tu Youyou, an organic chemist who worked to isolate and characterize active compounds from Chinese traditional medicines. She was able to isolate artemisinin from traditional medicines that had been used to treat malaria for centuries in China and received the 2015 Nobel prize in Physiology and Medicine for her work. (Tu Youyou is a women scientist who lived through the Cultural Revolution in China and made the discovery decades ago without any recognition. She has a remarkable story, look her up). There is also malaria prophylaxis available to help prevent one from contracting malaria in the first place. People generally do not take ACTs prophylactically because they are big guns that are reserved for bad cases of malaria. I was personally taking malarone (atovaquone/proguanil), which can cause nausea, vomiting, and insomnia. It only caused insomnia for me for a short period. Mefloquine, another popular prophylactic drug, is notorious for causing crazy dreams. Drug resistance to chloroquine, another popular drug, has developed around the world. Even strains resistant to ACTs have been isolated in Southeast Asia, which is a worrisome problem. Another challenge/drawback is that almost all the available drugs target the blood-stage of malaria infection, after the parasites have set up a productive infection and are reproducing like hell and causing all those shitty symptoms. Current research is focused on targeting the liver stage, when the parasites are at their most vulnerable.
Malaria has been around as long as man and has likely killed tens, if not hundreds, of millions of people. In fact, the mosquito has been recognized as the world’s second deadliest animal behind Homo sapiens in terms of lifeforms destroyed. Malaria is the prototypical tropical disease and is widespread in the tropics of Asia, South America, and Sub-Saharan Africa. In 2015, there were over 214 million cases of malaria worldwide and 438,000 deaths, mostly in Africa. Malaria is a classical disease of poverty and is responsible for hamstringing the economic livelihood of many poor countries, contributing to their being mired in poverty traps, a term popularized by the economist Jeffrey Sachs. For instance, malaria costs Africa $12 billion a year in healthcare costs, decreased tourism, and lost work potential.
Ok, back to my project and what I am doing in Uganda. I spent my first few weeks in Bugoye hiking to drug shops in mountainous villages, where I worked with drug shop owners to track their sales of anti-malarial drugs. I had to identify the rough locations of all the drug shops in the sub-county, hike out to them, inventory their drugs, and leave them with a form that would enable them to track their sales of anti-malarial drugs for one month (August 1 – August 31, 2017). Our goal was to collect data and hopefully induce >80% of the drug shop owners to return their completed sales tracking forms by offering them an incentive of 10,000 Ugandan shillings (~$2.50). Dr. Boyce also gave me a GPS so I could log the coordinates of each drug shop. To accomplish this, I had previously drafted two forms while I was still in the USA: an Initial Visit Form that I would use to inventory the supplies of the drug shops when I visited them, and a Sales Tracking Form that I would leave with the drug shop owners.
I visited my first drug shop on July 19, 2017 with Dr. Boyce and my guide Robert. Dr. Boyce wanted to do some trial runs with me before he left on July 21. Furthermore, Dr. Boyce had access to a car in Bugoye, so he drove us to some of the farther-flung villages in the sub-county. I’m glad he did, it would have taken me an entire day, dawn to dusk, to reach some of these villages, fill out the form, and return to Bugoye Health Center III.
I was accompanied on my adventures by my guide Robert, a native of Bugoye sub-county. He spoke English very well and knew all the local languages (the main dialect is called Lukonjo). He knew the sub-county’s terrain like the back of his hand and took me on all the secret shortcuts. He also knew a staggering amount of people all over the sub-county, everyone would stop and say hi to him and chat with him while we were walking to the villages. He was also a part-time guide in Rwenzori Mountain National Park and knew so much about the flora and fauna of the area. Robert put yours truly to shame while hiking, even though he came down malaria while we were in the middle of our fieldwork. He just popped some coartem and soldiered through our strenuous days. When I asked him how often he (a healthy, strong, active man in his 20’s) came down with malaria, he told me 2-3x a year.















We ended up visiting about five hard-to-reach villages using the car before Dr. Boyce had to leave. The rest I would have to get to on foot. But first, I had a weekend in Mbarara to look forward to. I hitched a ride with Dr. Boyce back to the big city on Friday.
An unexpected surprise was waiting for me in Mbarara. I woke up in my lodgings, the Little Woods Inn, on Saturday morning and decided to check Facebook to see what was going on back in the USA. As I was scrolling through my feed, I noticed that my old friend from the NIH, Jacob Fohtung, had posted a status that he was in Uganda. Excited, I messaged Jacob telling him that we should meet up if convenient before heading to breakfast. While I was eating, Jacob replied that he would love to meet up, that he was in Mbarara, and that he was staying at a lodge called the Little Woods Inn. I stared at his message for a moment, my mouth slightly open as I reflected on how bizarre it was that such a vast world could simultaneously be so small. I then messaged him that I was in the same lodge and was having breakfast and that he should join me. A few seconds later, Jacob came out of the lounge area and made a beeline for me in the dining area. I had walked past him without even seeing him. We had a lovely time catching up over breakfast. Jacob was in Uganda until the end of August working for a start-up incubator called CAMTech (based in Cambridge, MA and affiliated with MGH). He had been sent to Mbarara to collaborate with MUST and help some fledgling healthcare start-ups get on their feet.

I spent the rest of my weekend hanging out with Jacob. I also got to meet the people staying at the MGH guest house, which was right across from the Little Woods Inn. They were a nice group of people ranging from undergrads to residents to nurses to attending physicians. There was even a physician there who was head of the pediatric oncology division at MGH.
Week 3 (July 24-30) – Left To My Own Devices
I headed back to Bugoye alone on Sunday evening to prepare myself for the busy week to come. I would be spending the week hiking to as many villages as possible and trying to track down village drug shops and their owners with Robert. We had to visit all of the drug shops in the sub-county before August 1 (Tuesday the following week) because we needed to get the sales tracking form to them before the month commenced.
On Monday, I made my first foray into the hills facing the health center where I was living. I was headed to some nearby villages (about an hour away). My schedule for the week generally went like this: I would wake up with the sun around 7am to the sound of the roosters crowing and the birds chirping. After eating breakfast, I would meet up with Robert around 9am. We hiked up into the hills and to the villages we had targeted for the day. The hikes were of varying difficulties and durations, and we also had wide variation in the numbers of drug shops in the villages. We generally got back around 2pm, though sometimes we were out till 5pm. I would pack some snacks for us and we would ask the catering staff at the health center to prepare us a meal for when we returned. We lucked out because there was a special BIMI training at the health center this week, so they hired a team of cooks who were more than happy to save a portion for Robert and me. Otherwise, the health center does not usually have a catering service.





















 For some reason, whenever I come to a fork in the road in the woods, unbidden my mind hearkens back to the wistfulness and melancholy I associate with “Stopping By Woods on a Snowy Evening” by Robert Frost. No internet at the moment, but I think it goes something like this:
For some reason, whenever I come to a fork in the road in the woods, unbidden my mind hearkens back to the wistfulness and melancholy I associate with “Stopping By Woods on a Snowy Evening” by Robert Frost. No internet at the moment, but I think it goes something like this:
Whose woods these are I think I know
His house is in the village though
He will not see me stopping here
To watch his woods fill up with snow.
My little horse must think it queer
To stop without a farmhouse near
Beside the woods and frozen lake
The darkest evening of the year.
He gives his harness bells a shake
To ask if there is some mistake
The only other sound the sweep
Of easy wind and downy flake.
The woods are lovely, dark, and deep
But I have promises to keep
And miles to go before I sleep
And miles to go before I sleep.
As a reminder, our goal was to visit as many drug shops as we could on foot this week. When we got to a village, we had to locate the actual drug shop and the shop’s owner (easier said than done, as I’ll tell you) so we could explain the study to them, inspect their stock of anti-malaria drugs, and give them the sales tracking form. We encountered significant challenges in achieving these goals. I had experienced some of these challenges the previous week, but I’m choosing to talk about them here because last week was only a trial run and I had a car so it was way easier to get to the villages. My guide Robert was instrumental throughout this travail; without him, I would have just gotten lost in the mountains and utterly failed to collect any useful data.
The first and foremost challenge was that the drug shop owners were simply not at the drug shop when we visited the villages. Businesses do not have regular hours in the village trading centers. Generally, the shop owners spend the morning in the fields husbanding crops and the afternoon running their shops. However, sometimes stores would be open in the morning and not the afternoon, so there really was no discernible pattern and we were at the mercy of the whims of the drug shop owners. Even if we called ahead and notified the village chairmen that we were coming on a certain day and to tell the drug shop owners to expect us at a specific time, we would arrive at the village and find that the drug shops were still not open and the owners were nowhere to be found. Indeed, there were quite a few times when we could not track down the drug shop owner (despite our best efforts) and returned to the health center empty-handed. Here are some of the reasons why drug shop owners were unavailable:
- Owner was far away working in the fields and their phones did not have reception
- Owner was in Kasese re-stocking
- Owner was away attending a funeral of a relative. Sadly, this was the reason multiple times.
- Drug shop had recently moved to another village/sub-county or had closed down. There seems to be a lot of flux in the drug shops, quite a few of them had gone belly up or moved to neighboring Maliba sub-county, and it was difficult to find this out until we got to the actual villages. For instance, the one drug shop in a village called Ndughutu West closed down literally the week we went there. We ended up hiking to the village about four times without luck and eventually learned that the proprietor was at a nearby hospital and had sold all her wares to pay for her son’s operation to repair a hernia.
A second challenge was distrust in the community. Some of the drug shop owners thought we were inspectors coming to shut them down (many of the drug shops were not registered) and would avoid us. For instance, one drug shop owner got wind that we were coming and hid from us in her fields. When we finally got her phone number from a relative and called her, she still mistrusted us and actually turned her phone off so we couldn’t contact her. We returned to the village repeatedly looking for her without success. We eventually won her over by asking another drug shop owner in the same village to intercede for us and convince her intransigent compatriot that we meant no harm.
A third challenge was that we overlooked a number of anti-malaria drugs in our initial visit and had to re-visit a bunch of drug shops. At first, I began all my interviews with the open-ended question “show me all the drugs you use to treat malaria.” The drug shop owners would immediately pull out some pills and show me. I assumed that the pills were all they had (we were sitting in these dirty little shops in these poor villages, after all), so I noted them and thought I was finished. However, as I visited more shops, I saw evidence that made me suspect that I might be missing some anti-malaria drugs. For instance, I walked into one shop and was surprised to see a woman sitting on the ground with a needle in her vein, receiving IV drugs. When I asked her and the drug shop owner what she was receiving, they told me she was getting IV quinine, an anti-malaria drug. In the past stores I had visited, they had showed me their quinine tablets, but not any vials with quinine in liquid form for IV use.


I soon realized that I had missed an entire market for IV anti-malaria drugs as well as liquid quinine syrup for children. For some reason, when I asked drug shop owners to “show me all the drugs you use to treat malaria,” they would only show me pills and not IV drugs or syrups. I don’t know if this was due to a translation error or if IV drugs and syrups are not classified as “drugs” in Uganda. When I realized this midway through the week, I quickly added more drugs to the sales tracking form and began to budget time to re-visit drug shops so I could give them the updated tracking form and re-inspect their inventory. I also changed tactics and began to ask the drug shop owners if they had specific drugs from an exhaustive list of anti-malarial drugs I had compiled previously. This annoyed a lot of the shop owners but it was worth it. My new method enabled me to identify several drug shops that carried anti-malaria drugs that were uncommon in Uganda because they were so expensive.
I learned the hard way that open-ended questions don’t always yield the intended result, that meanings can get lost in translation, and that one must find an arbitrary balance between brevity and specificity. For instance, I have recently been making deliberate attempts to include open-ended questions into the verbal tactics I employ when I interview and counsel people. A common critique of my performance in simulated patient encounters during my first year of medical school was that I tended to put words into my patient’s mouths when the patient wouldn’t respond fast enough. People who observed me advised me to slow down and ask more open-ended questions and let the patients describe their situation in their own words without my adjectives coloring their testimony. Of course, these suggestions are valid and I took them to heart. However, upon experiencing the vagaries of vagueness in the field, I adopted a hybrid technique where I would begin with an open-ended question and follow up with specific, pointed questions.
Furthermore, I wish I had heeded my tendency to perseverate and build fail-safes into my systems so I could cover all my bases. My first draft of the sales tracking form had included every single anti-malarial drug that I could fit onto the page. I was later counseled to pare the form down because it was unlikely that the drug shops would have all those drugs and that having such a complicated form might confuse the drug shop owners. Acknowledging that concision is a virtue and that my field experience was virtually nil, I simplified the form and left checkboxes for only the two most common drugs on the sheet, along with a section for Others so drug shop owners could write in other drugs. This became problematic because many drug shops carried more than the two drugs that we had predicted to be most common. Again, this instance taught me that finding a way to blend and balance two ostensibly incongruous viewpoints (i.e., brevity vs. verbosity) enables one to achieve the best possible result. The art inherent in science. You can pay for school, but you can’t buy class. This is why I’ll never amount to anything.



I learned many lessons about global health and field research this first week. For one thing, I quickly realized that Ugandans wiggle their eyebrows silently to respond “yes” to questions. I would ask them questions and they would just wiggle their eyelids without saying anything, which confused me for a while. On a more serious note, here is a list of lessons that I learned from my experiences in the field:
Lessons reiterated/learned:
- Patience is a virtue
- Flexibility/improvisation are key
- Be observant and ready to learn on the fly and turn on a dime
- Be okay with less than optimal results (apparently getting >80% of the drug shop owners to return their forms is publishable) or even failure
- Expectations vs. reality
- Information and meaning can get lost in translation
- Balance concision and specificity when interviewing people
- Try not to let your frustration show. It was quite physically challenging to get to some of these villages, and I admit I got a bit frustrated when I made the hike all the way out there and was not be able to find the drug shop’s owners despite Robert and I trying everything possible to notify them that we were coming and trying to track them down once we got there.
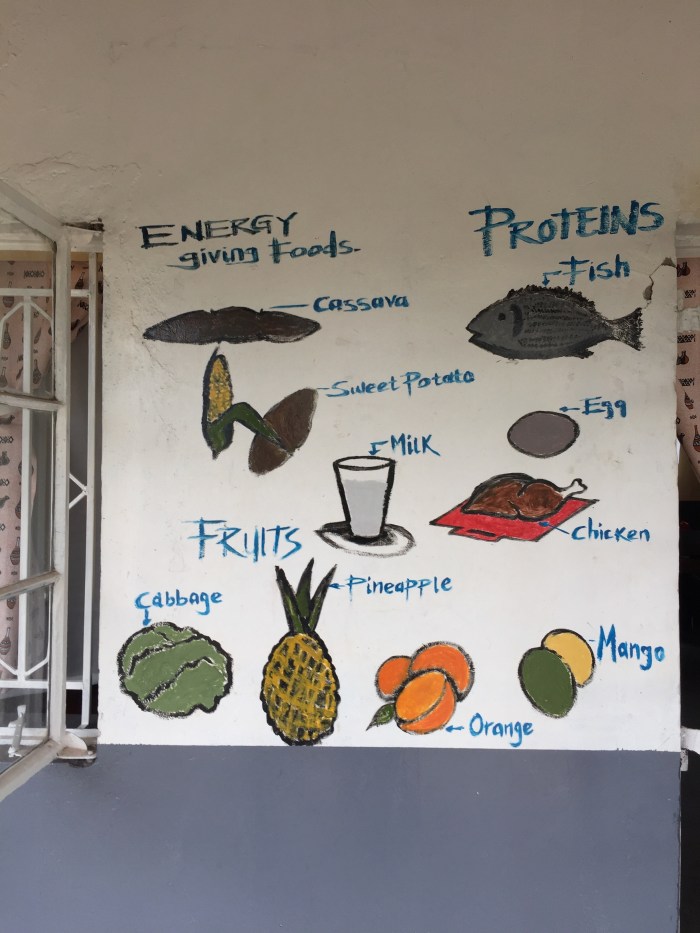
Sorry for subjecting you to such tedium. Let’s talk about Uganda’s food! Ugandan food mostly consists of carbohydrate staples that are grown by subsistence agriculturalists. It is hearty fare but most of it is tasteless and sits like a brick in your stomach after you finish your meal.



























I was also able to observe some of the civil infrastructure in the area. Bugoye sub-county is located near the Rwenzori mountains and has many large rivers. The Ugandan government has been trying for decades to harness the hydroelectric potential of the rivers. Uganda’s first dam was built in the 1960’s near the Kilembe mines (which are now closed) in the Kasese district and was used to power the operation of the mine. The dam and its associated pipes were made by the Canadians. In the 2000’s, another dam system was constructed by the Norwegians which featured large, open-air cement channels.












Well, that concludes the work week for my third week in Uganda and my first week flying solo without Dr. Boyce. I finally was able to take my first pleasure trip within Uganda, though I didn’t end up going that far. On Friday, I headed north up the road from Bugoye Health Center III for about 12 km to the Equator Snow Lodge.

The Equator Snow Lodge is located a few minutes from one of the entrances to the Rwenzori Mountains National Park, a World Heritage Site where visitors can go hiking, climbing, and bird watching. The Snow Lodge is a luxurious and expensive (by Ugandan standards) lodge near the park. There are only four cabins, all of which are huge. It is peaceful and quiet up there. I was lulled to sleep by the chirping of insects at night and awoken at dawn by the lilting song of birds.





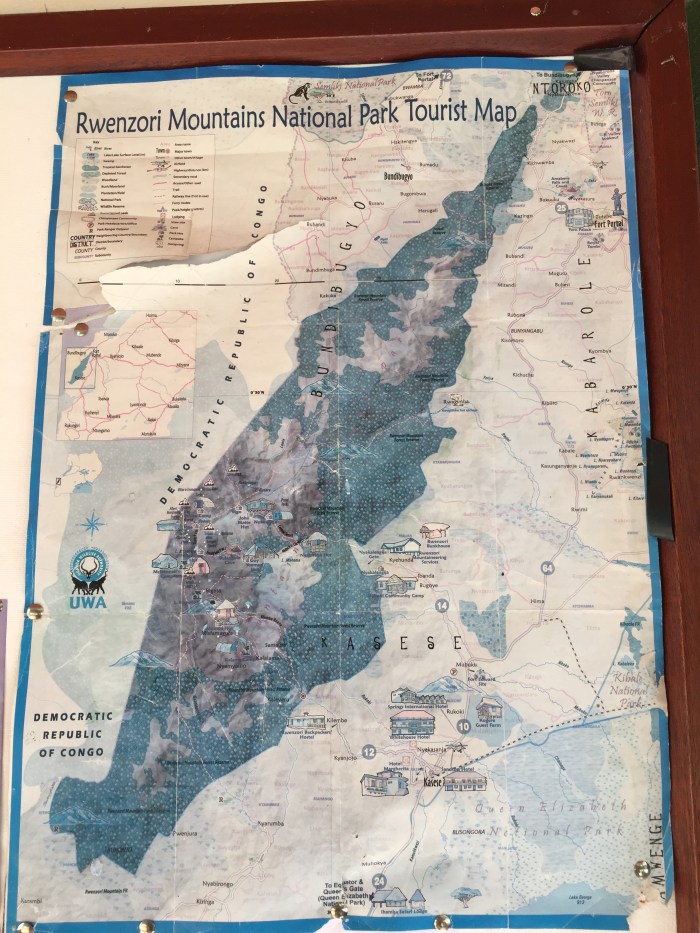


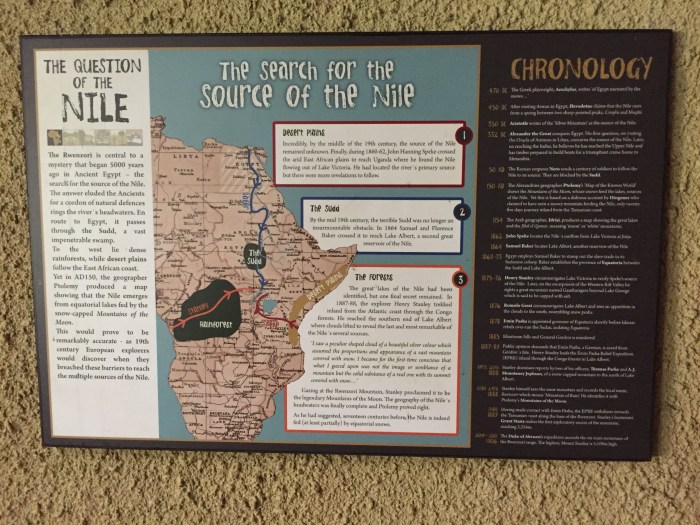
The Rwenzoris are also known as the Mountains of the Moon and have an incredibly interesting backstory that was detailed in placards on the walls of the lodge. I really enjoyed the placards, they were very well-written and would encourage you to read them if you can zoom in and make them out.


I spent the rest of my Friday exploring the area around the lodge. I had heard that the Snow Lodge had a hot spring and was excited to soak in it. I was incredibly disappointed to learn that the hot spring was more like a lukewarm puddle.





On Saturday morning, I arranged for a guide to take me up a nearby hill so I could see the snow-capped peaks of the Rwenzoris. I didn’t enter the park because I had to pay an exorbitant fee and I knew I didn’t have the time to actually climb any of the Rwenzoris. So I settled for a chance to glimpse the Mountains of the Moon.










All in all, my first pleasure trip in Uganda was a bit of a flop. The Snow Lodge was expensive and frankly not worth the money. The food was fine but overpriced. My cabin was drafty at night because there was no glass on the windows and the hot water echoed the lukewarm nature of the “hot springs,” so I didn’t shower and just went to bed. The hike up the hill to see the peaks was strenuous and not terribly enjoyable. The trail was steep and muddy and I almost fell a couple of times, which would not have been fun given the steepness and muddiness. And the view of the Rwenzori peaks that I was promised was sadly obscured by the clouds. The only part of the trip that I fully enjoyed was when I found the Mbuku river and lay on a rock for about an hour, staring at the sky listening to the sound of the water rushing by and letting my mind wander.
I was pooped after the hike on Saturday morning but had already made up my mind to walk back to the health center in Bugoye with my loaded pack. This was a distance of about 12 kilometers, from beyond one of the furthest village in the sub-county. I was determined to do this and not hire a car to take me back because I wanted to experience how difficult it was for the local populace to get to the health center on foot, deeming that the weight of my loaded pack approximated that of a large baby or adolescent child. The walk down was fine at first but the sun came out in the afternoon as I was walking and beat down upon me. It became hard going, though I admit that I have many advantages to the locals. For one, I am taller than most people here and have longer strides, I am certainly better fed and rested and not driven by desperation because my child is sick. Nonetheless, this exercise helped me appreciate the difficulties that the villagers face in getting to the health center on foot and how this might be a deterrent for them until the disease gets really bad (and by then it is often too late).
I spent my Sunday back in the field with Robert. We were both motivated to finish visiting the drug shops before the deadline of August 1. The local’s schedule benefited us this time, Robert told me that the shops are usually open on the weekend because the drug shop owners (who usually live near or next to their shops) open them on the weekend to do business. So, I pretty much spent the entire weekend hiking.
It wasn’t until this weekend spent exploring the Rwenzori’s that I hit upon the perfect title for my blog post. I was spending my free time re-visiting a seminal book in my development as a budding physician. The book is Mountains Beyond Mountains: The Quest of Dr. Paul Farmer, A Man Who Would Cure the World by Tracy Kidder. This book introduced me to Paul Farmer and is one of the identifiable objects that put me on the medical path in the first place. I would highly recommend the book to anyone. If you are in interested in medicine, poverty, social justice, infectious diseases, global health, or just want to read a good book (it won a Pulitzer), then pick up this one. I promise you won’t be disappointed.
While reading the book, I realized that Bugoye and Uganda shared many similarities to Cange and Haiti (former colonies of Western imperialist powers, endured periods of intense strife and war, impoverished with high rates of disease). In terms of surface qualities, Bugoye is also very mountainous like Cange, which is what made me think of the title. When I was heading to the villages, I would climb one mountain and realize that there was yet another mountain behind it that I had to climb to reach my destination. Similarly, the moment I thought I had overcome one challenge in the field, another would take its place (cut off one head, two more shall take its place. Anyone?). For me, these proverbial mountains beyond mountains also represent the conundrums of infectious disease and global health, which are rooted in some of the age-old constants inherent to the algorithm of human society (e.g., poverty, injustice, and cruelty) and are foremost among the challenges of our time, or indeed of all time. These puzzles are impossibly complex and can engage one for a lifetime, which is exactly why I am interested in them.
The second part of my title reflects my love for travel. Peripatetic means traveling from place to place, usually for work, never rooted down to a location for long. I have been blessed with chances to travel extensively this summer, and indeed in the past year. My desire to see the world is recent. I didn’t travel very much when I was young, though I did travel quite a bit within the USA during high school for national fencing tournaments and spent a few summers in Taiwan when I was a young child. But this was just for necessity, and I didn’t necessary look forward to or enjoy it like I do now. It wasn’t until college that I was bitten by the travel bug and began to understand the term “wanderlust.”
My realization that I possessed a visceral yearning to see the world coincided with the kindling of my interest in medicine in my freshman year. Indeed, part of the reason why I am so interested in infectious diseases and global health is because travel is such an integral component to these fields. One of the fascinating things about infectious diseases that originally drew me to the field is how deadly pathogens have the potential to spread all over the globe in an astonishingly short amount of time and indiscriminately devastate the health and economies of societies. I realized that I wanted to study, experience, and understand the world, both at a microscopic and macroscopic. Similar to how I want to fathom how cells are governed and how proteins fold into thermodynamically-stable conformations and how elementary particles coalesce into atoms, I want to see how people spend their daily lives frittering away their limited time on earth, understand their worldviews and their answers to fundamental questions of existence and how they weave the disparate threads of individuals into cohesive societies, and experience their food and drink and music and dance, those crystallizations of culture. I want to see as much of this little insignificant rock hurtling through space toward certain destruction in £500,000,000 years that I happen to be stuck on, striving for the ideal of cosmopolitanism and not just seeing the parts of the world that are top destinations for tourists. Simply put, I am striving to fundamentally understand life while I am yet full of it myself, before my fleeting flame is extinguished forever.
Anyway, that’s it for part one. Thanks for reading.
– Lawrence